Unified Clinical AI Intelligence Across the Trial Lifecycle
The trial lifecycle was built as a sequence of handoffs, not a system — and intelligence is lost at every one. Innovo Copilot is one connected AI layer that closes the loop, from protocol to live monitoring.
The regulatory bar has moved
ICH E6(R3) (FDA-adopted Sept 2025) and the FDA's first AI guidance demand risk-based, technology-enabled, auditable oversight.
Risk-based, quality-by-design oversight
The first GCP overhaul in three decades — explicitly embracing modern technology, data governance, and risk-based monitoring.
AI must be credible & risk-assessed
A risk-based bar for the credibility of any model that informs a regulatory decision.
Research → Author → Monitor
Three modules, one loop. Every phase feeds the next — intelligence never gets lost in the handoff.
Research
Evidence & feasibility, before you design.
Author
Protocol, plans & documents, governed.
Monitor
Risk-based, live, protocol-aware oversight.
The questions sponsors keep asking
“We amended three times. What were we designing against?”
“Why didn't you see this coming?”
Protocol design is made in a vacuum — and feasibility is a guessing game dressed up as diligence.
Know before you design
Design grounded in evidence — prior trials, real-world data, literature, and your own organizational memory — before the protocol is written, not after the third amendment.
What good looks like
Every design decision backed by a source.
- Disease & mechanistic evidence — the landscape and rationale, synthesized from the literature
- Competitive design benchmarks — how prior and ongoing trials were actually designed
- Patient-grounded feasibility — real-world data validating I/E criteria and enrollment
- Organizational memory — your knowledgebase and the learnings already inside it
From scattered sources to a structured synopsis
Inputs: PubMed & literature, CT.gov / AACT, 300M+ real-world data records, rare-disease databases, your sponsor knowledgebase.
- Objectives & design rationale
- Primary & secondary endpoints
- Validated I/E criteria — patient-grounded, not assumed
- Enrollment & timeline benchmarks
- Competitive landscape summary
The questions sponsors keep asking
“We've been in governance for six weeks. How is the protocol not final?”
“We spent a million dollars fixing something that should never have been in the protocol.”
Authoring is still cut-and-paste at scale — and amendments are operational emergencies in slow motion.
Authoring that converges, not drags
Evidence-backed drafting and AI quality control turn governance from a six-week bottleneck into a convergence — and catch the design flaws that become million-dollar amendments.
Protocol authoring
Generate and refine evidence-backed sections directly from your knowledge base.
Governance review
Consolidate, summarize and prioritize reviewer feedback; surface conflicts early.
QC agents
Check accuracy, consistency and regulatory alignment (FDA / EMA) before sign-off.
Study-startup docs
Auto-draft ICF, CRF and DMP from the approved protocol, in any language.
Amendment cascade
Push a protocol change to every related document automatically.
Design optimization
Flag elements prone to deviation using prior-trial patterns — before finalization.
The questions sponsors keep asking
“The FDA found it — why didn't we?”
“When did you know the trial was off track, and why are we only hearing about it now?”
Monitors fly blind until they're standing in the site — and portfolio risk is invisible until it's a timeline problem.
Continuous, risk-based, grounded in the plan
Oversight that surfaces risk as it emerges — tied to its timeline impact, with the right action attached. The closed loop ICH E6(R3) now expects.
One site risk score
EDC, CTMS, eTMF & training unified — no manual pulling.
Risk surfaced early
Connected to enrollment, queries, deviations & readiness.
Action attached
Breach → CAPA → verified closure, automatically.
Grounded in the plan
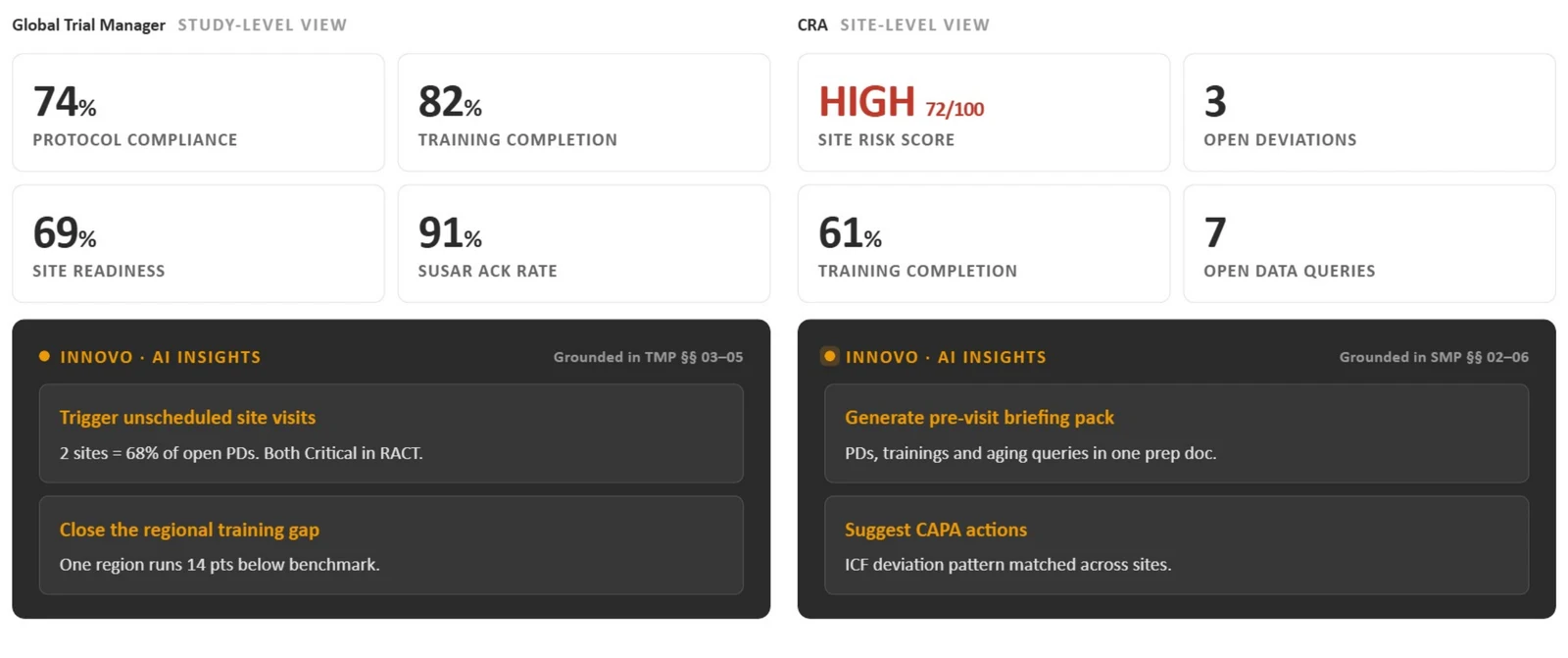
Every insight references the exact TMP / SMP section. Role-based dashboards for Global Trial Managers and CRAs.
What each role sees — grounded in their plan
The Global Trial Manager gets a study-level view; the CRA gets a site-level view. Both run on the same live signals — and every AI insight cites the exact TMP / SMP section it is grounded in.
From signal to verified resolution
Safety breach → CAPA → verified closure
Breach detected → matched to RACT → CAPA triggered → effectiveness verified.
- ~80% faster breach-to-CAPA
- 100% of protocol deviations tied to a RACT domain
Pre-visit briefing → MVR → site closeout
Open findings → pre-visit pack → site visit → MVR pre-filled.
- 3–5 hours saved per CRA visit
- ~70% of the Monitoring Visit Report pre-filled
Powered by Innovo AI
Innovo Copilot grounds every output in your organization's curated clinical knowledge base (ClinThink) — historical protocols, SOPs, regulatory context, and relevant external research.
Unlike generic LLM tools, it does not generate content in isolation: structured clinical ontology, study-specific context, and embedded quality-control agents validate alignment with CDISC standards, regulatory guidance (FDA, EMA), and internal governance. All outputs are traceable, version-controlled, and fully reviewable — transparency, human oversight, and regulatory defensibility across the clinical lifecycle.
The loop, closed — and the scale we've earned
Not a point solution — the whole loop
Manual / status quo
- 3–5 hr visit prep
- Days to breach detection
- Open CAPAs, no closure check
- Siloed systems
- Sponsor finds it first
Other AI tools
- Protocol authoring only
- No monitoring module
- No RACT-to-CAPA loop
- Sponsor-side only
- Proof of Concept demos
Innovo Copilot
- Protocol → live monitoring
- CRO + sponsor layer
- Automated CAPA closure
- EDC + CTMS + eTMF integrated
- Proof of Outcome model
Frequently asked questions
What does Innovo Copilot author?
The Author module supports every phase of document creation — from early planning to final reporting:
- Protocol Authoring: draft key sections with AI-powered suggestions and evidence-backed insights
- Study Governance Review: summarize reviewer input, trace feedback history, and align with regulatory and internal standards
- Study Startup & IRB Packages: create submission-ready documents using reusable templates and pre-approved content
- Study Conduct & Closeout: auto-update linked documents after amendments and generate CSRs and Lay Summaries with minimal manual input
Whether you're starting a new trial or closing one out, Copilot keeps your documents accurate, aligned, and ready to move forward.
Who is Innovo Copilot for?
Innovo Copilot is designed for sponsors and CROs working across multiple trials. It enables collaboration between clinical, regulatory, and operations teams, reducing bottlenecks and manual rework.
How does Innovo Copilot ensure accuracy?
Innovo Copilot grounds every output in your organization's curated clinical knowledge base (ClinThink), integrating historical protocols, SOPs, regulatory context, and relevant external research.
Unlike generic LLM tools, Innovo Copilot does not generate content in isolation. It applies structured clinical ontology, study-specific context, and embedded quality control agents to validate alignment with CDISC standards, regulatory guidance (FDA, EMA), and internal governance requirements.
All outputs are traceable, version-controlled, and fully reviewable — ensuring transparency, human oversight, and regulatory defensibility across the clinical lifecycle.
How does Innovo Copilot ensure compliance and data security?
Innovo Copilot is built for enterprise clinical environments with strict data governance requirements.
Your data remains within your secure environment and is never used to train public AI models. The platform operates within a controlled architecture with encryption standards, audit trails, and enterprise-grade security safeguards.
All activity is logged and traceable to support compliance, system validation, and inspection readiness — ensuring sponsors and CROs can leverage AI while maintaining full control over their clinical data, intellectual property, and regulatory obligations.
What results can teams expect?
By supporting the full loop, Innovo Copilot helps teams:
- Close breach-to-CAPA ~80% faster, with verified closure
- Avoid 2–3 amendments per study through evidence-grounded design
- Cut protocol deviations by 40–50%
- Expand CRA capacity 30–50% with pre-visit packs and pre-filled MVRs
What makes Innovo Copilot different from other AI tools?
Innovo Copilot is built specifically for clinical teams — not adapted from general-purpose AI. What sets it apart:
- The whole loop — protocol to live monitoring, not authoring alone
- A tailored AI agent framework supporting authoring QC, monitoring, and CAPA closure
- Unique RAG delivering highly accurate results across therapeutic areas
- Multilingual study-startup documents for global trial readiness from day one
- Purpose-built for real-world clinical workflows — the entire document lifecycle from drafting to submission
Proof of Outcome — not just Proof of Concept
We'll baseline your current monitoring metrics and prove the impact on a real study workflow.
Request a Demo